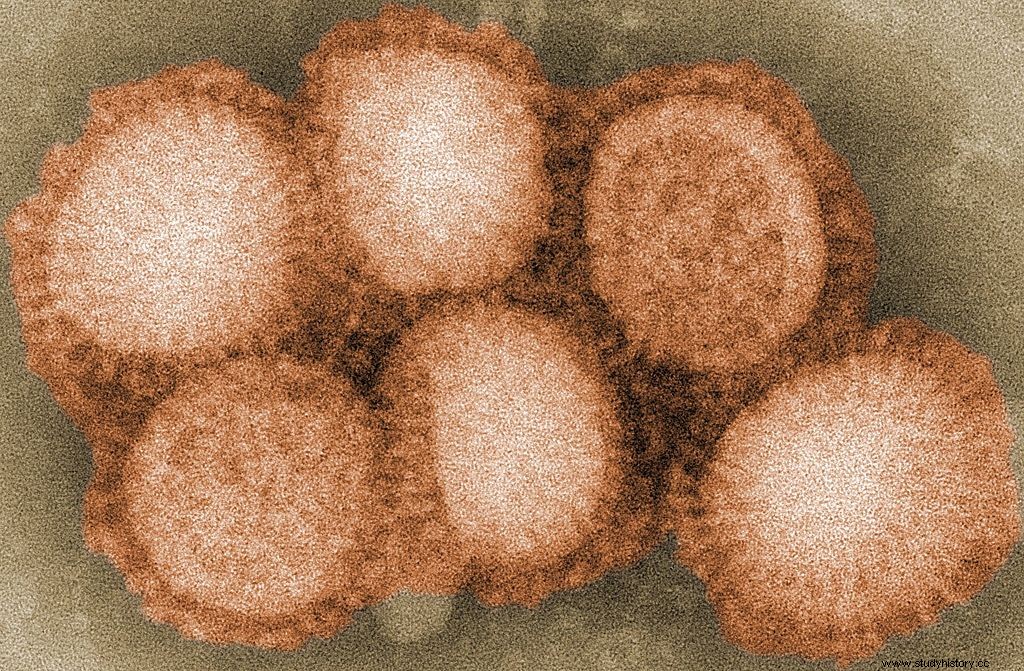
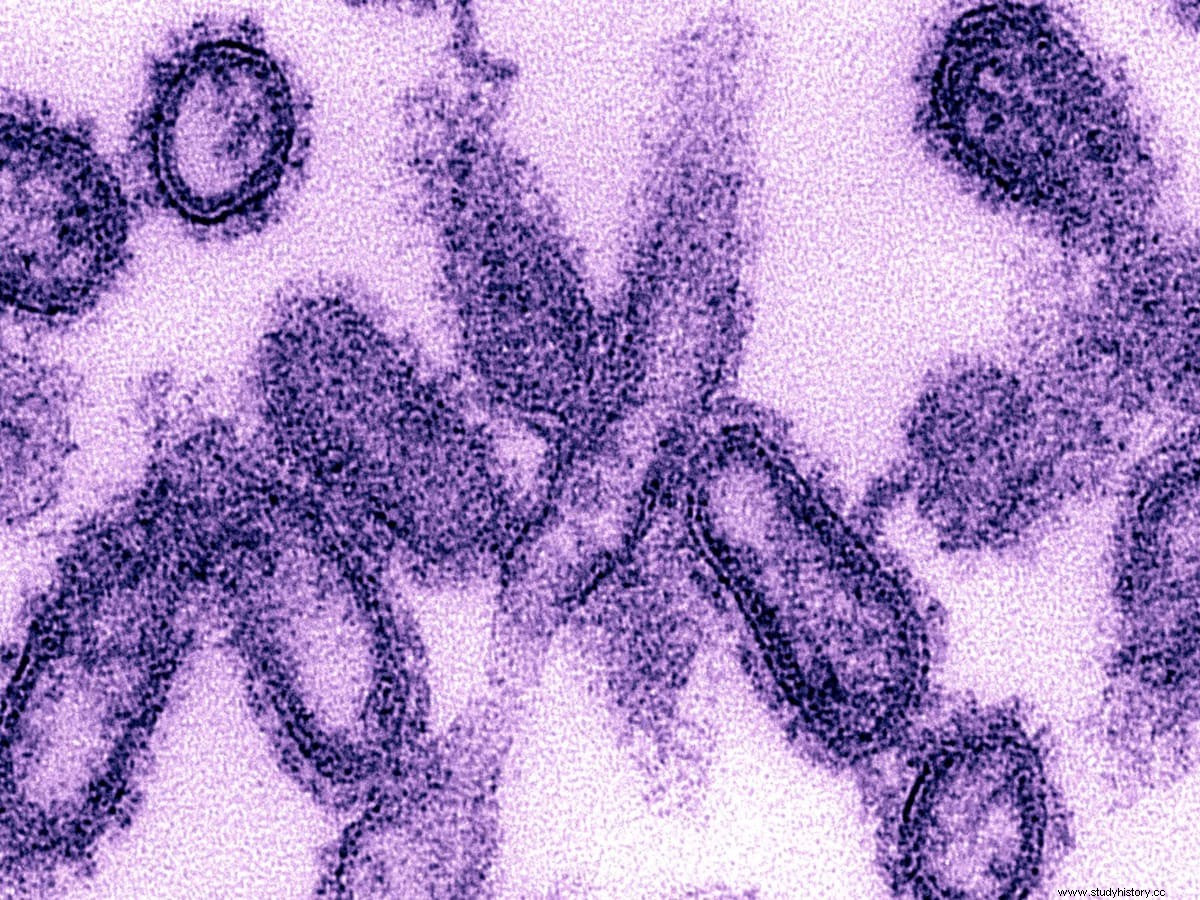
The Spanish flu, also known as the 1918 flu pandemic, was a rare form of the H1N1 virus. It lasted from February 1918 to April 1920 and infected 500 million people - about a third of the world's population at that time - in four waves in a row. The death toll is estimated to be between 20 million and 50 million, although it is estimated to be between 17 million hard-core to 100 million, making it one of the deadliest diseases in human history.
The first observations of illness and death were recorded in the United States (Kansas) in March 1918 and in April in France, Germany and the United Kingdom. To maintain morale, World War I inspectors reduced these first reports. Newspapers were free to report the effects of the epidemic in neutral Spain, such as the tragic death of King Alfonso XIII, and the news gave a bleak picture of Spain as a major offensive. This created the term "Spanish flu". Historical details and diseases are insufficient to determine the origin of the epidemic, with varying degrees of geographical location.
Most flu outbreaks occur very young and very old, with a high survival rate among them in the middle, but the Spanish flu epidemic has led to higher mortality than expected in adults. Researchers provide several explanations for the high mortality rate from influenza in 1918, including the harsh six-year climate that disrupted the spread of infectious diseases and increased the risk of waterborne disease. Some studies have shown that the virus is particularly deadly because it creates a cytokine storm, which destroys strong immune systems in adults. On the other hand, an analysis from medical journals from the 2007 epidemic found that the virus was no longer more aggressive than previous influenza strains. Instead, malnutrition, overcrowded medical camps and hospitals, and poor hygiene, all exacerbated by the recent war, encouraged the spread of the virus. This defeat for the disease killed many of the victims, often after a long death row.
The Spanish flu of 1918 was the first of three viruses caused by the H1N1 virus; the last was the swine flu epidemic in 2009. The Russian flu in 1977 was also caused by the H1N1 virus, but it mainly affected young people.
First wave, early 1918
The epidemic was marked as the one that began on March 4, 1918 with the recording of the trial of Albert Gitchell, a military cook at Camp Funston in Kansas, USA, even though there had been cases before him. The disease was discovered in Haskell County in January 1918, prompting local physician Loring Miner to warn the American Public Health Service Journal. Within a few days, 522 men in the camp reported being ill. On March 11, 1918, the virus had reached Queens, New York. Lack of security measures in March / April was later criticized.

When the United States entered World War I, the disease spread rapidly from Camp Funston, a large military training base in the U.S. Expeditionary Forces, to other U.S. armies and European camps, and became a pandemic in the Midwest, East Coast, and French ports in April 1918, and we reaches the western front in the middle of the month. It soon spread to France, Britain, Italy and Spain, reaching Breslau and Odessa in May. After the signing of the Brest-Litovsk Treaty (March 1918), Germany began to release Russian prisoners of war, who then brought the disease to their country. It arrived in North Africa, India and Japan in May, and shortly afterwards it may have traveled to the rest of the world as cases were recorded in Southeast Asia in April. In June, a disease was reported in China. After arriving in Australia in July, the tide began to recede.
The first flu pandemic broke out in the first quarter of 1918 and was minimal. Mortality was not above the normal range; In the United States, ~ 75,000 1918 people died of influenza in the first six months of 63,000, compared to ~ 1915 1918 deaths in the same period in 1918. In Madrid, Spain, less than a thousand people died of influenza between May and June 900,000. There was no isolated isolation in the first quarter XNUMX. The first wave, however, caused significant disruption in World War I military operations, with three-quarters French soldiers, half British troops and more than XNUMX XNUMX German soldiers ill.
Dangerous Second Wave, August 1918

The second wave began in the second half of August, and probably spread to Boston and Freetown, Sierra Leone, by ship from Brest, where it was probably brought by US or French troops trained in the Navy. From the Boston Navy Yard and Camp Devens (later renamed Fort Devens), about 30 miles west of Boston, other U.S. military bases. They were soon harassed, and soldiers were sent to Europe. Assisted by military action, it spread over the next two months to all of North America, then to Central and South America, and even to Brazil and the Caribbean by ship. On July 30, the Turkish government recognized its first cases against other soldiers. From Freetown, the epidemic continued to spread across West Africa along the coast, rivers and colonial railways, and from railways to remote communities, while South Africa bought it in September on ships taking back members of the South African Native Labor Corps back from France. . From there it spread to South Africa and beyond the Zambezi, reaching Ethiopia in November. In September 1918, New York City witnessed its first influenza death. The Philadelphia Liberty Loans Parade, held in Philadelphia, Pennsylvania, on September 15, 28 to promote the Government's commitments from World War I, resulted in the death of 12,000 people in 1918 after a massive outbreak of the disease spread to visitors to the exhibit.
From Europe, the second wave passed through southwestern Russia — formerly northeastern, and was brought to Arkhangelsk by intervention from northern Russia, and then spread through Asia after the Russian Civil War and the Trans-Siberian Railway, reaching Iran (where it spread) in the holy city of Mashhad), and later in India in September, as well as in China and Japan in October. The ceasefire celebration of 11 November 1918 also caused riots in Lima and Nairobi, but by December the tide had abated considerably.
The second wave of catastrophic floods in 1918 was more deadly than the first. The first wave was similar to the cold; those most at risk were sick and older, while the younger and healthier were more likely to recover. October 1918 was a month of high mortality throughout the epidemic. In the United States, ~ 292,000 1918 deaths were reported between September-December 26,000, compared to ~ 1915 40,000 in the same period in 15,000. The Netherlands reported 1.1 1918+ deaths from influenza and respiratory infections. Bombay reported that 12.5 20 people out of 1918 million people had died. The influenza epidemic in XNUMX in India was catastrophic, with an estimated XNUMX-XNUMX million deaths in the last half of XNUMX alone.
Why was the second wave so dangerous?
The dreaded scale of the 1918 flu epidemic - known as the "Spanish flu" - is difficult to understand. The virus infected 500 million people worldwide and killed an estimated 20 million to 50 million victims - more than all soldiers and civilians killed during World War I.
While the global epidemic lasted for two years, a large number of deaths were reported in the worst three months, especially in the autumn of 1918. Historians now believe that the deadly effects of the "second wave" of the Spanish flu were due to a virus transmitted by the military . When the Spanish flu first appeared in early March 1918, it had all the symptoms of the flu season, even though it was a highly contagious and powerful flu. One of the first recorded cases was Albert Gitchell, an American military chef at Camp Funston in Kansas, who was hospitalized with a 104-degree fever. The virus spread rapidly through the deployment of troops, home to 54,000 1,100 soldiers. By the end of the month, 38 soldiers had been hospitalized and XNUMX had died of pneumonia.
Third Wave of 1919
In January 1919, a third wave of Spanish flu swept across Australia, killing 12,000 1919 people after the removal of prisons, and then spread rapidly to Europe and the United States, where they remained until the spring of June 1919. It strongly affected Spain, Serbia, Mexico and the United Kingdom, resulting in the deaths of hundreds of thousands of people. It was much heavier than the second wave, but still more deadly than the first wave. In the United States, external eruptions occurred in other cities, including Los Angeles, New York City, Memphis, Nashville, San Francisco, and St. Louis. Louis. The total U.S. death toll was tens of thousands in the first six months of XNUMX.
Fourth wave
In the spring of 1920, a fourth wave broke out in isolated areas, including New York City, Switzerland, Scandinavia, and other islands in South America. New York City alone reported 6,374,1919 deaths between December 1920 and April 1918, nearly double the first wave in the spring of 1920. Other U.S. cities include Detroit, Milwaukee, Kansas City, Minneapolis and St. Louis. Peru experienced a tidal wave in the late 1919s, and Japan had another from the late 1920s to 1920, the last coming in March. In Europe, five countries (Spain, Denmark, Finland, Germany and Switzerland) recorded the highest number between January and April XNUMX.
The main origin of the Spanish flu
China
In 1993, Claude Hannoun, a leading Spanish influenza specialist at the Pasteur Institute, claimed that the original virus may have originated in China and then spread to the United States near Boston and spread to Brest, France, European stadiums, Europe and the rest of the world, with soldiers. Allies and sailors as major distributors. Hannoun sees various options, such as Spain, Kansas and Brest, as possible, but not impossible. In 2014, historian Mark Humphries argued that recruiting 96,000 1917 Chinese workers to work behind the British and French lines could be the source of the epidemic. Humphries, from Memorial University of Newfoundland in St. John's, holds his conclusions about the recently obtained records. He found the archaeological evidence that a respiratory disease affecting northern China (where workers had left) in November XNUMX was identified the following year by Chinese health authorities as the Spanish flu. However, no tissue samples from today's comparison survived. However, respiratory diseases were reported in parts of the route that workers had taken to Europe, which also passed through North America.

One of the few regions in the world that seems to be less affected by the Spanish flu pandemic is China, where a number of studies have shown that the flu season in 1918 was mild. Although this is challenging due to lack of data during the warlord period, see Worldwide. This has led to speculation that the Spanish flu epidemic has appeared in China. The incidence of influenza can be explained by the number of Chinese who have previously received the flu vaccine.
A report published in 2016 in the Journal of the Chinese Medical Association found no evidence that the 1918 virus was introduced to Europe by Chinese and Southeast Asian soldiers and personnel and instead found evidence of spread in Europe before the epidemic. A 2016 study suggested that the low incidence of influenza (estimated at one in a thousand) among Chinese and Southeast Asian workers in Europe means that the deadly 1918 flu pandemic would not have occurred in these workers. Another proof that the disease is still transmitted by Chinese workers is that workers entered Europe via other routes without visible spread, which made it possible for them to be the first leaders.
Europe
Britain's largest military base and hospital camp in aptaples in France has been named by virologist John Oxford as the epicenter of the Spanish flu. His research found that in late 1916, the aptaples camp was hit by the onset of a new disease that caused high mortality that caused flu-like symptoms. According to Oxford, a similar outbreak occurred in March 1917 in Aldershot military camp, and later epidemics saw this outbreak as the same as the Spanish flu. The crowded camp and hospital in Etaples was an ideal place for the spread of respiratory infections. The hospital treated thousands of victims of gas poisoning, other war victims and 100,000 XNUMX soldiers who passed through the camp every day. And it was a pigsty, and chickens were often brought from nearby villages to feed the camp. Oxford and his team wrote that the previous parasite, with birds, mutated and migrated to pre-houses.
A report published in 2016 in the Journal of the Chinese Medical Association found evidence that the virus from 1918 had been circulating in European wars for several months and possibly years before the epidemic in 1918. Political scientist Andrew Price-Smith has published data from Austrian archives suggesting that influenza began in Austria in early 1917.
A 2009 study of influenza and other respiratory viruses found that Spanish flu deaths occurred simultaneously between the two months of October and November 1918 in all fourteen European countries analyzed, which did not match the pattern that researchers would expect if the virus appeared where preferably in Europe and spread. without.
Symptoms
Most infected people get only the usual symptoms of sore throat, headache and fever, especially during the first wave. During the second wave, however, the disease was more severe, often exacerbated by bacterial pneumonia, which was often the leading cause of death. This serious condition can lead to the development of heliotropic cyanosis, in which the skin may begin to develop two patches of mahogany on the bones of the grain and then over a few hours spread to a green surface, followed by black at the edges and then spread to the feet and body. . After this, death would follow within hours or days due to fluid-filled lungs. Other reported signs and symptoms include spontaneous mouth and nose, miscarriage in pregnant women, special odor, fallen teeth and hair, confusion, dizziness, insomnia, loss of hearing or smell, blurred vision and color vision. One commenter wrote:"One of the most common problems was bleeding from parts of the mouth, especially the nose, stomach and intestines. Bleeding from the ears and minor bleeding on the skin also occurred. Most of the symptoms are thought to be caused by cytokine storms.
Most of the deaths were caused by bacterial pneumonia, the most common common cold-related infection. The pneumonia itself was caused by normal respiratory bacteria, which managed to enter the lungs through the damaged bronchial tubes of the victims. The virus also kills people directly by causing severe bleeding and edema in the lungs. Modern studies have shown that the virus is particularly deadly because it causes a cytokine storm (an overdose of the immune system). A team of researchers identified the virus in the bodies of cold victims and infected animals. The animals experienced progressive respiratory failure and death from a cytokine storm. A strong immune response in adolescents was thought to be harmful, and weakened immune systems in children and middle-aged adults led to fewer deaths in these groups.
Mutation variants
The basic number of viral births was between 2 and 3. The settlements next to the great movement from the First World War accelerated the epidemic, and perhaps both increased transmissions and shift subsidies. War can also reduce resistance to the virus. Some believe that the immune system is weakened by malnutrition as well as by the aggression of chemical agents, which in turn increases the tendency. An important factor in the global flu epidemic is increased mobility. Modern transport systems make it easier for soldiers, sailors and public travelers to spread the disease. Another was the lies and denials of the government, so that people were unprepared to deal with the outbreak.

The difficulty of the second wave was due to the conditions during the First World War. In public life, natural selection prefers a smaller species. Those who are seriously ill live at home, while those who are less ill continue with life, preferring to spread the smaller type. In the trenches, natural selection was reversed. Soldiers with minor difficulties stay where they are, while black patients are sent to overcrowded trains in hospitals filled with fields that spread the deadly virus. The second wave began, and the flu spread rapidly throughout the world. As a result, during the epidemic of modern diseases, health authorities are searching for species that kill the virus when it reaches unstable areas of society. The fact that most people who received first-line treatment were no longer physically fit indicates that it should have been the same type of flu. This was demonstrated in a very significant way in Copenhagen, with a combined mortality of only 0.29% (0.02% in the first wave and 0.27% in the second wave) as a result of exposure to the first less lethal wave. Of all people, the second wave was the deadliest; the most vulnerable people are those who are like soldiers in the trenches - older people who were younger and fitter.
After the second tidal wave at the end of 1918, new cases suddenly fell. In Philadelphia, for example, 4.5,997 people died last week on October 16, but by November 11, the flu had almost completely disappeared from the city. Another explanation for the rapid decline in the incidence of the disease is that doctors are effective in preventing and treating pneumonia that develops after the victims became infected. However, in his 2004 book The Great Influenza:The Epic Story of the Deadliest Plague In History, John Barry stated that researchers had not found any evidence to support the claim. One theory is that the virus from 1918 quickly developed into a less deadly form. Such flu-like mutations are common:pathogenic bacteria tend to become harmless over time, as many of the most dangerous species tend to disappear. Other murder cases continued in March 1919, and one player was killed in the Stanley Cup final in 1919.
The impact of the Spanish flu, economically and socially
An estimated 40 million people, or 2.1 percent of the world's population, died of the great flu of 1918-20. If a similar epidemic occurs today, it will kill 150 million people worldwide. In the coronavirus and the major flu pandemic:Studies from the "Spanish flu" of the coronavirus' potential effects on mortality and economic activity (NBER Working Paper 26866), Robert J. Barro, José F. Ursúa and Joanna Weng study the cross - global variation in the number of deaths related to the outbreak, and the associated economic consequences.
The flu spread through three waves:the first in the spring of 1918, the second and deadliest from September 1918 to January 1919, and the third from February 1919 to the end of the year. The first two waves were amplified by the last years of World War I; the authors work to separate the effect of influenza on the death level from the effect of war. Influenza mostly kills older people in the absence of existing conditions, which has had a significant impact on the economy compared to the disease that affects young and very old.
Researchers analyzed mortality data in more than 40 countries, accounting for 92 percent of the world's population in 1918 and even the largest share of GDP. Mortality ranged from 0.3 percent in Australia, which set the target in 1918, to 5.8 percent in Kenya and 5.2 percent in India, which lost 16.7 million people in the three years of the epidemic. The flu killed 550,000 0.5 people in the United States, or 300,000 percent of the population. In Spain, 1.4 XNUMX deaths average XNUMX percent. There is no agreement on where the flu came from; met Spain because the media there were the first to report it.
There is little reliable information on how many are infected. The most common estimates, a third of the population, are based on a 1919 survey of 11 American cities; it may not represent the people of the United States, let alone the international community.
How did COVID-19 (2020) and the Spanish flu (1919) affect the Indian economy?
Economic growth and development are often shocking, which may be due to changes in society, the political economy, the environment, etc. This shock has an impact on access to any economy (Brainerd and Seigler 2003 Karlsson 2014). Epidemics are also a major threat to the economy, as these not only affect public health but also economic health. The history provides an overview of epidemics, epidemics and diseases that have occurred in the past, which results in a lasting impact on people's lives and economic activities (Boxmeyer 2006; Killingray 2003). Different nations and India were affected by the same disease in 1918, when the flu epidemic hit the world (García - Sastre and Whitley 2006; Gottfredsson et al. 2008; Karesh and Cook 2005).
The 1918 flu pandemic was a deadly virus caused by the H1N1 virus. It was one of the most widespread and deadly bombs ever seen by the world economy, threatening not only human lives but also society and trade-related activities. (Fargey 2019; Karlsson et al. 2014). Data from the World Economic Forum (WEF) indicate that around 500 million people contracted the flu - a third of the world's population at that time. The plague broke out in four consecutive waves between February 1918 and April 1920. Mortality was estimated at 2 percent of the world population and 5.2 percent of the population of India (World Economic Report 2020). Although the 1918 flu epidemic coincided with World War I, Figure 1 shows the death toll in India.
Compare COVID-19 and Flu 1918-19
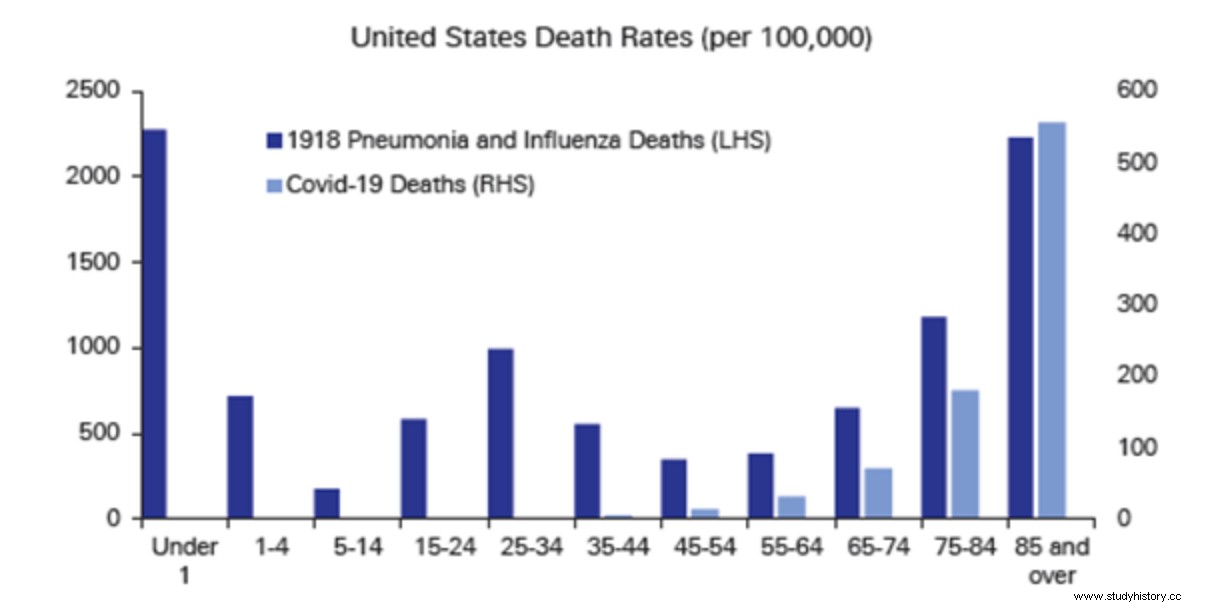
First, the number of patients varies. While the flu in 1918 killed an unprecedented number of 25-40-year-olds, while COVID-19 mainly affects people over 65, especially those with comorbidity. In particular, the death rate from influenza has risen to 8% -10% for young people compared to 2.5% mortality and the mortality rate for people aged 25 to 40 years is only 0.2% compared to a total mortality of 2.4%. Those aged 25-40 accounted for 40% of deaths due to influenza in 1918, while those aged 18-44 accounted for only 3.9% of COVID-19 deaths. Many countries survived the 1918 epidemic, and only the small Pacific islands (Soloman and Vanuata Islands) remain COVID-19 free. The mortality rate for pregnant women with Spanish flu was 23% -37% and 26% for those who survived but lost their babies, and the mortality rate for four pregnant women COVID -19 is unknown. The Spanish flu has led to massive disease in 25% -3 0% of the world's population, with over 50 million deaths, and COVID -19 has infected almost one million people 55 to date with 2 million deaths in the United States alone. COVID-19 cases are more than 11 million as of 16 November 2020, an increase of approximately 40% k from the previous month.
Second, these two diseases in different ways. While those with the flu died of secondary bacterial pneumonia, those with COVID-19 died of an overdose that led to many errors. 2 8 Acute respiratory disease (ARDS) can develop in both cases. As a complication of influenza, ARDS had a 100% mortality rate compared to a 53.4% mortality rate as a complication of COVID-19. The estimated economic impact of COVID-19 on the US economy is a decline of $ 5.76- $ 6.17 trillion in gross domestic product (GDP), based on Fitch Ratings and US GDP according to the World Bank. Economic data during the 1918 epidemic are scarce, but it was noted that Mexico lost $ 9 billion.
Things to learn from the Spanish flu pandemic to deal with the current COVID 19 pandemic
Since we are achieving an unparalleled record of one million cases in 10 days, it is time to stop, reflect, analyze and most importantly acknowledge that any attempt to combat the dreaded coronavirus attack has been in vain. While epidemiologists and world leaders tried to do their best, it was historical reports from the Spanish flu that warned of another wave of infectious disease. With the arrival of the second COVID-19 wave in India, it is fair to say that while the first Spanish flu wave killed an estimated 5,000 people in India, the second wave in September 1918 hit western India, and the estimated number of deaths is in one million million Indians. -12 to 18.
The current number of registered deaths is close to 1,70,000, most of us just a number. To put it bluntly, the total number of Indian soldiers martyred in the war in 1962 with China, and the three wars against Pakistan in 1965, 1971 and 1999 (Kargil), was less than 10,000 1. With the outbreak of 'epidemic fatigue' does not give 1 death, 70,000 19 XNUMX due to COVID-XNUMX a consistent response, as the deaths of our soldiers did. Part of our peace is due to the human tendency to pay more attention to the death of others than to others. Perhaps the survivors are reluctant to talk about an experience that seems impossible to hold or cure.
When we hear the news about vaccine shortages and the crowds at vaccination centers, let's try to understand the difference between making a vaccine and vaccinating more than 100 million people (about 75 percent of the population) to achieve any herd size. To understand the magnitude of the challenge, this number would be equal to the number of children collected for the five-year polio vaccine in India. Every year, nearly 2.3 million applicants under the leadership of 1,55,000 209 directors visit 20 million homes to offer Polio vaccine to children under 200 (19 million) under the age of five, cross-country skiing. With the nuances of individual COVID-2022 vaccines, temperature problems and dietary differences between injectable OPV drops compared to injectable potion, it is possible to look back at XNUMX before returning to the "normal pre-Covid" under the umbrella for protection against infection. It makes sense to minimize the celebration of the introduction of the vaccine, to extend safety measures such as social isolation, masking and active immunization.